Towards a feasible regulatory path for new PrEP products
HIV prevention is advancing, building on the success of treatment as prevention and once-daily oral pre-exposure prophylaxis (PrEP). However, additional prevention interventions are needed to meet the needs of individuals from diverse populations. The traditional regulatory path of two large randomized controlled trials demonstrating efficacy and safety is not feasible in many circumstances, given the success of the already available interventions. Specific challenges in design and analysis include the difficulty of demonstrating statistical superiority or non-inferiority due to the low number of events and identifying appropriate control populations against which to measure efficacy. Logistically, the number of participants needed to demonstrate superiority or non-inferiority may be too large and cost-intensive to be feasible. All stakeholders involved in HIV prevention research need to join in forging a feasible, scientifically sound path to demonstrate the efficacy and safety of new prevention interventions convincingly.The Forum HIV Prevention Trial Design Project will convene a series of public meetings to offer the community a powerful opportunity to review and discuss strategies together with all stakeholders to allow for less resource-intensive clinical trial options for new PrEP interventions' approval while maintaining scientific rigor. The Public Meetings' primary goal is to bring all stakeholders and different threads together, present the work to the general community in different regions of the world, and develop better strategies to advance the field further. These public meetings are intended to be practical and informal.
Background
Demonstrating the efficacy of the new intervention depends on comparing the impact of the intervention vs. no intervention on an outcome, in this case, HIV incidence. In PrEP research, we no longer can compare the HIV incidence in an intervention arm to a placebo. Instead, we seek to compare a new intervention – e., g. a long-acting antiretroviral – to the standard-of-care – Truvada. Because we expect a low incidence in both arms, we need to address an important question: was there HIV circulating in the population in which the trial was conducted or was there no HIV circulating because–e.g.most HIV infected individuals are on treatment, thus not able to transmit HIV to others in the community including those in the PrEP trial. If the latter is true, the low incidence in both arms will not reflect PrEP efficacy – it would simply confirm that treatment-as-prevention was doing what we expect it to do.
To address the question, we need to build convincing evidence that HIV would have been transmitted in the community in which trials are being conducted. We could then use this evidence to estimate what the incidence “would have been in the absence of PrEP”. If we estimate the incidence in a population similar enough to the trial participants to be around – e.g.– 4%, but the incidence in both trial arms is much lower – e.g.– 0.5%, we can be reasonably certain that both PrEP trial arms provided significant protection. How can we arrive at an estimate that characterizes what the incidence “would have been”?
The ideal comparator would be the exact same population enrolled in the trial, but somehow, by rolling back the clock, we could observe them again, this time around without them receiving the PrEP intervention offered to either of the two arms. We refer to this “ideal” -- not observable in real life– as the counterfactual (or contrary to fact). Thus, we need to look for other options to arrive at an estimate that comes as close as possible to the ideal counterfactual. For example, we could include a third arm in the study: a placebo arm. The placebo arm incidence would be the closest we can come to the ideal counterfactual– but that is not an ethical option because we now have a very effective standard-of-care for PrEP.Other options to estimate the counterfactual include surveillance data gathered for the relevant communities; a run-in cohort in which HIV incidence is observed before a trial is initiated; looking at those who were enrolled as HIV-uninfected but who subsequently seroconverted early on trial and could be confirmed acute HIV infected before starting PrEP dosing by the appropriate tests; looking at how recently those that test HIV-positive on screening were infected by using an HIV recency assay. Some of these options will be better than others to arrive at an estimate of HIV incidence for a population that is “similar enough” to the population under study. Counterfactual HIV incidence estimates that are derived from data as close as possible to the communities in the study will be the most convincing. Surveillance data, on the other hand, may be outdated and not completely representative of the trial participants. But, if several options all point to a similar estimate, we build more confidence that the estimated incidence is dependable.
Objective
The public meetings will facilitate understanding, commitment, and action from across the sectors and ensure the evidence for benefit and risk is convincing to everyone.The first set of meetings will provide background information on the regulatory framework for approval and capacity for innovation, the specific regulatory framework around PrEP interventions, and bring everyone up to speed on the main concepts. The second series will be based on discussion and deliberation among stakeholders to inform decisions on specifics in trial design and analysis for diverse populations. These discussions will focus on issues regulators, particularly the U.S. Food and Drug Administration (FDA), European Medicines Agency (EMA), and African Regulatory agency, are particularly interested in receiving broader community input on. These events will highlight the importance of information exchange by ensuring everyone that plays a role in the field is included.
The public meetings will further reinforce the importance of community involvement in achieving the goal of evolving consensus and recommendations regarding a paradigm shift in the regulatory path for novel PrEP interventions.
Proposed Format
The HIV Prevention Trial Design Project Planning Committee, comprised of stakeholders from across the sectors, will contribute to planning for the Forum HIV Prevention Trial Design Public Meeting Series. The planning committee will develop the topics, program, and agenda for each public meeting, including identifying panelists, presenters and distributing the invitation. It will also create and disseminate the informational package that explains the counterfactual concept for participants.
The series of web-based and in-person meetings (when possible) will take place in 2020 and 2021. The programs will be developed with input from stakeholders across the sectors (community, regulators, industry, academia, etc.).
Expected Outcomes
- Increased understanding of clinical trial design complexities and consideration of an alternative approach, such as the counterfactual approach to estimating HIV incidence in communities where HIV prevention trials are being conducted.
- Recommendations on how to address the issues related to clinical trials, current approaches, and design to facilitate less resource-intensive clinical trial options leading to approval of new PrEP interventions.
Public Meetings Planning Committee
| Member | Organization |
| Frank Amort, PhD | EATG |
| Rachel Baggaley, MBBS, MSc | World Health Organization |
| Gus Cairs, M.A. | PEI, (the PrEP in Europe Initiative); EATG |
| Sinead Delany-Moretlwe, MD | University of the Witwatersrand |
| Fiona Greenhalgh, MA, MSc | EATG |
| Beatriz Grinsztejn, MD, PhD | Oswaldo Cruz Foundation |
| David Haerry | EATG |
| Jeremiah Johnson, MPH | TAG |
| Grace Kumwenda, M.A. | Pakachere Institute |
| Regine Lehnert, MD | Federal Institute for Drugs and Medical Devices |
| Kenneth Mayer, MD | The Fenway Institute/ Harvard Medical School |
| Veronica Miller, PhD | The Forum for Collaborative Research |
| Jean-Michel Molina, MD, PhD | French National Agency for AIDS Research |
| Charu Mullick, MD | U.S. Food and Drug Administration |
| Jeffrey Murray, MD, MPH | U.S. Food and Drug Administration |
| Jim Rooney, MD | Gilead Sciences, Inc. |
| Kathleen Squires, MD | Merck |
| Vani Vannappagari, MBBS, MPH, PhD | ViiV Healthcare |
| Roger Tatoud, PhD | International AIDS Society (IAS) |
| Tamar Tchelidze, MD, MPH | The Forum for Collaborative Research |
| Stephaun Wallace MOL, MS, PhD | HIV Vaccine Trials Network |
| Mitchell Warren, B.A. | AVAC |
| Ntando Yola, B.A. | Desmond Tutu Health Foundation |
Educational Materials
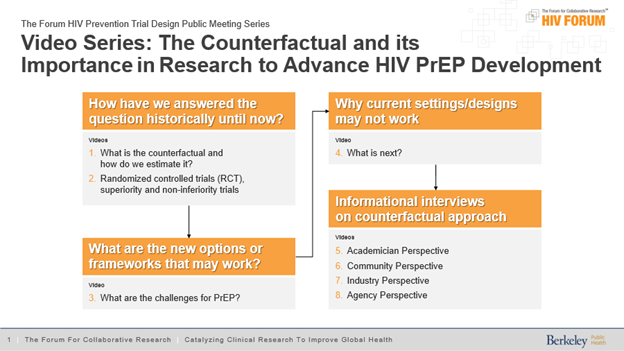
Educational materials in video and text form will be developed to facilitate discussions and have participants up to speed and engage in strategic discussion. Those materials can be accessed here. Please find the flow chart of video informational materials below.